In recent years there has been a noticeable increase in the utilization of stereotactic delivery techniques in radiation therapy. The continuing COVID epidemic has accelerated this trend even further. This increased prevalence has brought attention to the quality assurance necessary to accurately and safely deliver treatments that target very small volumes with large amounts of radiation.
AAPM Task Group 218 (TG-218) recommends true composite patient specific quality assurance (PSQA) for IMRT and VMAT deliveries “provided the QA device has negligible angular dependence or the angular dependence is accurately accounted for in the vendor software.” [1] They further state that these measurements “should not be performed using the PC [Perpendicular Composite] delivery method which is prone to masking delivery errors.”
Certain stereotactic treatments, such as Single-Isocenter Multiple-Target (SIMT) rely on precise combinations of gantry, collimator and couch rotations. Faught, et al, showed that for SIMT treatments, differences in 1.0 degree in gantry, collimator and couch rotations could result in maximum changes to V100% of 18%, 33% and 5% respectively, [2] highlighting the increased need to follow TG-218 QA recommendations to prevent the possibility of potentially catastrophic errors.
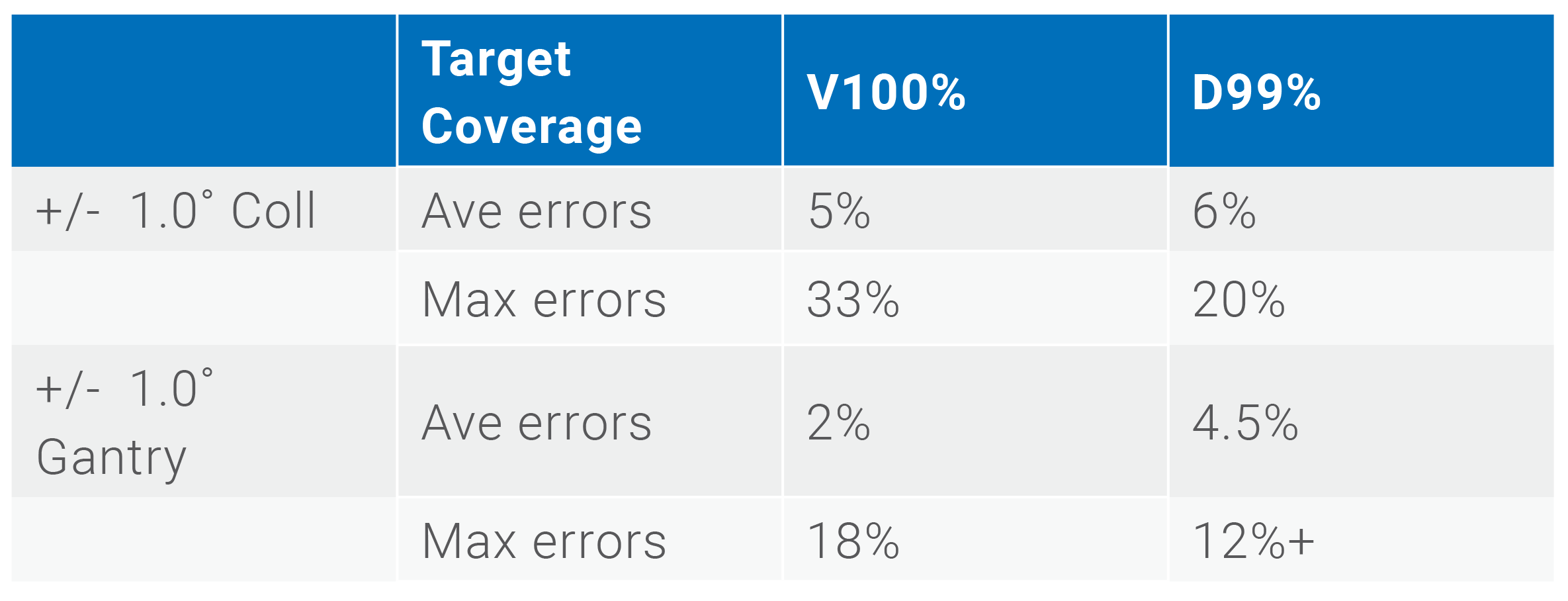
Summary of data from Faught et al publication2
The most efficient method of performing stereotactic PSQA is an array that utilizes either ion chambers or diodes of sufficient resolution. A new device utilizing a CMOS detector has also recently been introduced. With multiple devices available for SRS quality assurance, care should be taken in determining which provides the most effective QA to ensure safe and precise treatments for a facility’s patients. Specifically, clinicians involved in performing these critical measurements need to determine whether a solution meets the requirements for TG-218 true composite measurements. While some arrays claim TG-218 compatibility, in stereotactic deliveries that means being able to manage angular corrections for gantry and couch rotations simultaneously, including vertex fields, something only one available device can accomplish.
The Sun Nuclear SRS MapCHECK diode array features a patented method for determining the incident angle of radiation through differing responses of detector pairs. No additional equipment (such as a gantry angle sensor) is needed, reducing setup complexity and the possibility of error introduction from additional devices. The array is fully compatible with evaluating delivered dose with gantry and couch geometries as specified in the patient plan, including vertex deliveries. With 2.47 mm detector spacing and unmatched 0.48 mm detector resolution, the SRS MapCHECK provides film equivalent results that support the additional TG-218 recommendation of tighter tolerances for SBRT such as 3%/1mm or 2%/1mm. Additionally, since nearly all SIMT plans include lesions on multiple planes, the included QA Setup Tool helps users determine the optimal setup(s) to complete QA in as few deliveries as is possible.
For sites seeking commissioning guidance for their SRS program, Culcasi et al, recently published a standardized set of structures, planning goals and delivery requirements for five increasingly complex stereotactic cases. Modeled after the AAPM Task Group 119 test suite published in 2009 for IMRT Commissioning, the cases include VMAT plans featuring a single arc, two coplanar arcs, a full arc and vertex half arc, and four non-coplanar arcs. [3] The authors used the Sun Nuclear SRS MapCHECK as part of their validation, measuring dose distributions with the planned couch, collimator and gantry angles. They specifically noted that the array featured diodes with an active measurement area of 0.48 x 0.48 mm, making it compliant with AAPM Task Group 101 recommendations for stereotactic detectors to have a spatial resolution better than 1 mm. [4]
SRS MapCHECK is the only array that meets TG-101 and TG-218 recommendations, and can adequately replace film and mimic the full patient delivery in true composite form. Click hereto learn why SRS MapCHECK is becoming the gold standard for film-less SRS and SBRT QA.
Neal Miller, MBA
Neal Miller is a Product Marketing Manager at Sun Nuclear, the leader in quality assurance solutions for radiation therapy and diagnostic imaging. Neal has worked as a medical device marketing professional for over 20 years, mostly in the radiation therapy quality assurance field, bringing timely information to the market about latest technologies and best practices.
References
[1] | M. Miften, et al "Tolerance limits and methodologies for IMRT measurement-based verification QA: Recommendations of AAPM Task Group No. 218," Medical Physics, pp. e53 - e83, 2018. |
[2] | A. M. Faught, et al, "Re-examining TG-142 recommendations in light of modern techniques for linear accelerator based radiosurgery," Medical Physics, no. 43, pp. 5437-5441, 2016. |
[3] | R. Culcasi, et al, "Stereotactic radiosurgery commissioning and QA test cases—A TG-119 approach for Stereotactic radiosurgey," Medical Physics, pp. 1-12, 2021. |
[4] | S. H. Benedict, et al, "Stereotactic body radiation therapy: The report of AAPM Task Group 101," Medical Physics, vol. 37, no. 8, pp. 4078 - 4101, 2010. |
This article was originally published in the European Federation of Organisations for Medical Physics (EFOMP) Fall 2021 Newsletter. Find the full newsletter here.